HCG on cycle – To use or not?

Intro
The use of HCG on cycle or TRT is somewhat of a recent trend.
There are many benefits that can be gained by doing so, but also some key considerations.
The goal of this post is to give you a clear understanding of how HCG influences our hormones, the effects it produces and to put you in a position where you can make an informed decision as to whether to include it in your cycle or not.
What is HCG
HCG or Human-Chorionic-Gonadotropin is largely a female hormone, produced by the placenta during pregnancy.
Males also produce HCG, albeit in much smaller quantities than females. Men produce more LH (luteinizing hormone) which stimulate the Leydig cells in the testicles.
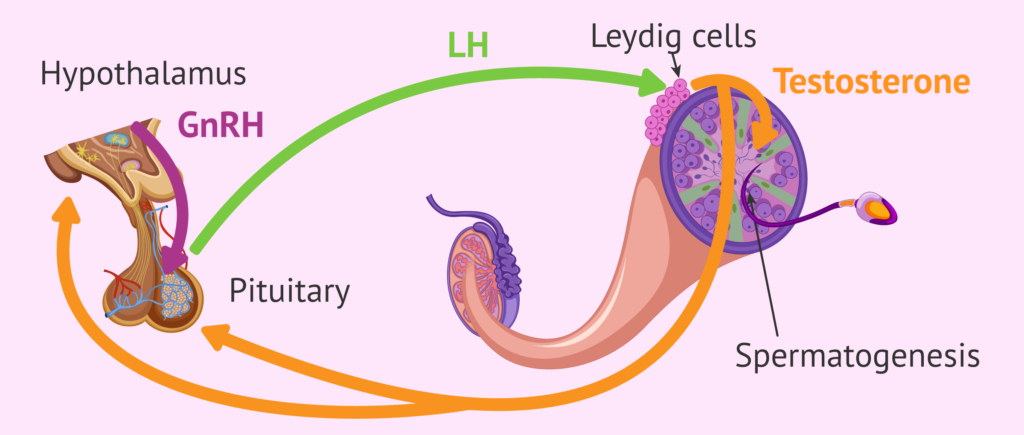
In men, HCG can simulate and play the same role as LH (luteinizing hormone) – which sends a signal to the testes to produce testosterone and sperm.
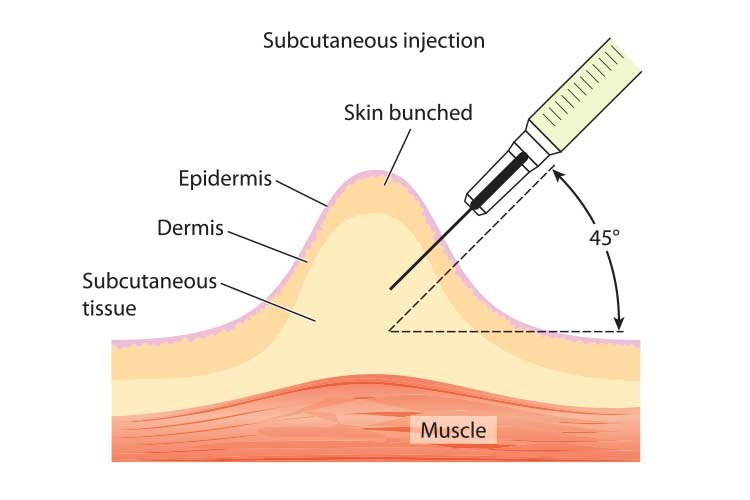
HCG is typically available in 5000iu vials of freeze-dried powder which can be reconstituted with bacteriostatic water making it available for subcutaneous injection (typically into belly fat).
Why use HCG on cycle
Using HCG on cycle has many benefits.
Firstly, the use of HCG on cycle allows the testes to function as normal, that would otherwise be shut down due to a downregulation of the HTPA (Hypothalamic–pituitary–adrenal axis) via, the introduction of exogenous androgens.
Your HTPA is responsible for regulating the amount of androgens produced by the testicles. When you introduce a surplus of androgens exogenously, this process shuts down leading to a vast reduction of Gonadotropin-releasing hormone (GnRH) resulting in the pituitary gland not releasing LH (luteinizing hormone), further leading to testicular shutdown and atrophy.
Testicular shutdown and atrophy are very often associated with decreased orgasm sensation and reduced penile sensitivity.
It’s speculated that prolonged periods of shutdown can cause oxidative stress and scar tissue formation which can permanently damage the testicles, possibly compromising long term fertility.
So by using HCG on cycle, you are allowing the natural process to continue.
When your HTPA is shutdown, StAR (Steroidogenic acute regulatory protein) is also shutdown. This plays a critical role as a transport protein that regulates the process of turning cholesterol into endogenous steroid hormones.
Why is that important?
The surplus of cholesterol that ISN’T being used as building blocks to create hormones is left to circulate in the blood and may increase the rate of plaque formation in arteries.
The HTPA is also responsible for the producing various neurosteroids, namely DHEA, pregnenolone and progesterone, which play a big role in libido, mood and general sense of well-being.
If your plan is to PCT after a cycle, then HCG on cycle throughout can make the recovery process much smoother and faster.
HCG on cycle allows you skip the step in the PCT process where you’re attempting to ‘wake up’ your testicles and get them to go from 0 to 100 in order to produce testosterone again. This makes the process of restoring your endogenous production and fertility easier.
19-nor derivatives and HCG
The group of steroids in the 19-nor category are particularly suppressive to the point where they can ‘override’ HCG and still cause suppression and shutdown.
HCG on cycle kept my testicles normal size and semen volume normal on a cutting blast of 250mg Testosterone + 250mg Masteron per week with 750iu HCG.

Then post blast, I was cruising on 140mg Testosterone propionate + 90mg Masteron enanthate with 750iu HCG, per week.
During this time my body was responding as it should to the HCG, keeping my testicles normal size and preventing atrophy.
I then added 70mg (10mg/day) of trenbolone acetate for four weeks as an experiment. Within two weeks it was as if I’d stopped responding to the HCG, I started to have a dull ache in my testicles which to me is the sign they are shut down and about to atrophy.
The volume of my semen also halved.
I understand that everyone responds differently to various compounds but this to me was first hand evidence and highlighted the suppressive power of 19-nor derived steroids even in small doses!
Endogenous LH vs. HCG
Endogenous luteinizing hormone has a half-life of 20 minutes, this is because it’s released in pulses when the hypothalamus detects that it needs to create hormones.
On the other hand, injectable HCG has a half-life of 24-36 hours and a total active life of around 5 days.
G-Protein downregulation
Exogenous HCG binds to the LHCGR (Luteinizing hormone choriogonadotropin receptor) and due to the long half life may cause overstimulation, resulting in G-protein downregulation.
This is the signal that is sent to the testicles to produce testosterone once HCG has bound to the LHCGR.
To what extent exogenous HCG causes the process to downregulate is highly individualistic.
Generally people fall into one of two groups. One group may have no issues using HCG continuously at moderate doses throughout an AAS cycle, and the other group may have to cycle it to allow for periods of re-sensitization.
I’m in the latter group unfortunately and have most success when following a 2 weeks on, 2 weeks off protocol.
Dosing HCG on cycle
Dosing can depend on many factors, but I believe the minimum amount to use is 500iu per week split into two subcutaneous injections roughly 3 days apart – Monday and Thursday for example.
The most common dose to maintain fertility, sexual sensation and prevent testicular atrophy on cycle is 750-1000iu per week.
Either split into 3x 250iu shots, or x2 500iu shots.
For a guide on how to mix and store HCG, check out this post
If your cycle includes a 19-nor derivative (Nandrolone, Trenbolone, Trestolone), then personally I wouldn’t bother with HCG on cycle due to their highly suppressive nature.
Instead opting for a more intensive restoration process post-cycle as either part of a PCT or cruise would be a better option.
HCG as part of a PCT
The use of HCG as part of a PCT will greatly increase the probability of restoring optimal natural function post-cycle.
Four weeks following the last injection of AAS, you can begin using HCG at 2000-3500iu per week.
Waiting four weeks is important as it allows most of the longer esters to fully metabolise and clear from the body.
If your cycle only included shorter esters (propionate/acetate), you can begin using HCG after just two weeks.
Typically dosing is a lot higher than during a cycle. This is because the intent is to re-establish the signal between your HTPA and testicles that has been shut down while exogenous androgens were present.
Drawbacks of HCG
While for most there are undoubtedly more benefits than drawbacks to using HCG on cycle, there are still a few things to consider.
Increased estrogenic load
HCG tends to increase Estrogen more disproportionately to Testosterone, so if you’re a high aromitizer then this is something to bare in mind.
The Estrogen it produces is intra-testicular, which is makes AI’s ineffective at lowering it.
To adjust for this, you can simply lower your testosterone dose to account for the increased estrogen caused by the HCG.
Cost, preparation
While HCG is currently quite cheap at £20 per 5000iu vial here in the UK. It’s still an extra expense on top of everything else at the end of the day.
Also, while the preparation doesn’t take very long. It’s still a tedious process and pain in the ass.
Making the personal call to use HCG on cycle
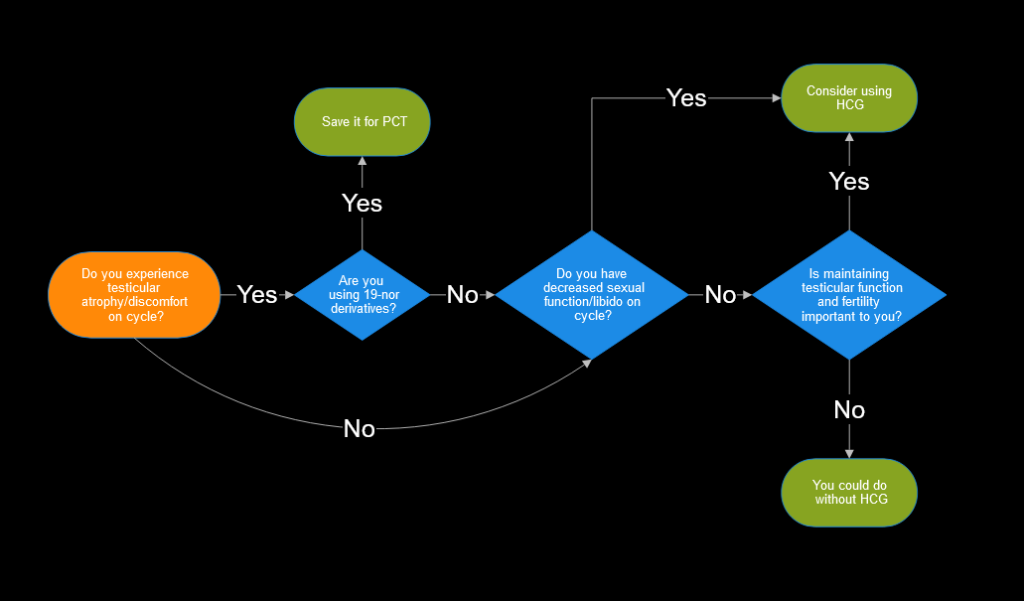
So should you use HCG on cycle or not?
Well ultimately it’s a call only you can make, however I’ve put together a flow chart to help you make the decision.
Click to expand.
Related Posts
Keys to retaining maximum muscle post-cycle
How to realistically get a better physique than 99% of the population.
